Cuboid Photos, Images, Video & Pictures
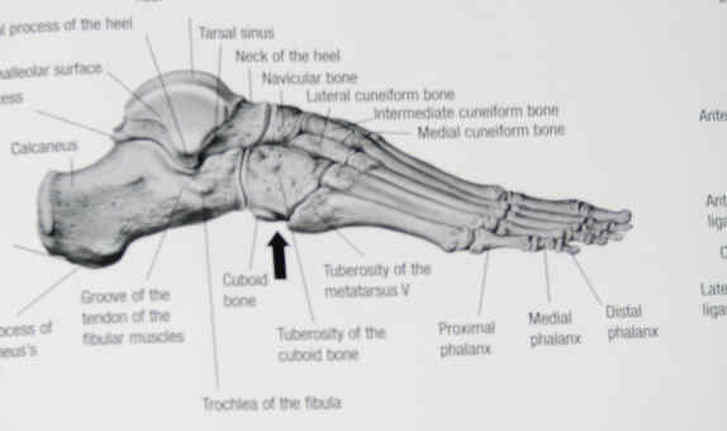
Lateral view of right cuboid. Arrow points to the right cuboid, looking from the outside of the right foot.

Top view of left cuboid.
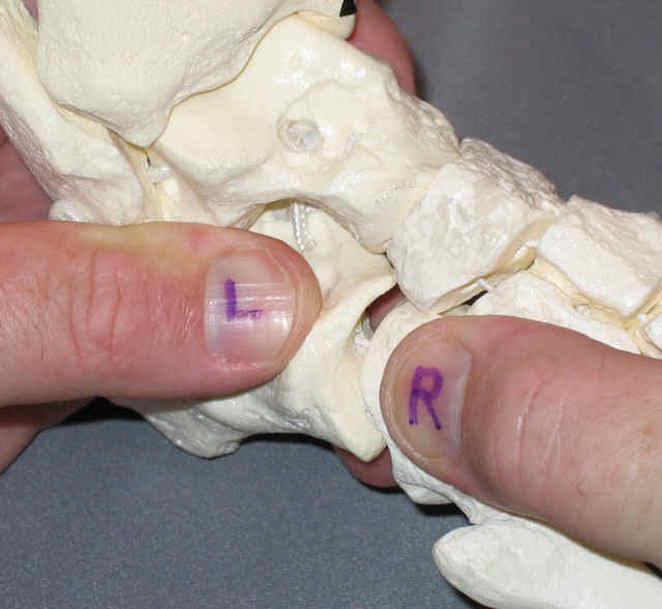
Outside view of left foot. Left thumb is on the calcaneus (heel) the largest bone in the foot. right thumb is on the cuboid. I am distracting the joint and you can see the very curved joint surface. the "take home message" is that the calcaneus is much larger and has a powerful influence on the cuboid. It is very important to evaluate mobility of the calcaneus and restore normal mobility when able, as opposed to just restoring mobility of the cuboid, in presentations of cuboid syndrome. The goal here is prevention of recurrence, not just relief of acute symptoms.

Lateral view of right foot with intact cuboid and solitary cuboid below.

View from bottom of foot. Note the curved surface where the calcaneus (large bone top left) joins the cuboid, whereas other bones that connect to the cuboid have a fairly flat (planar) shape.